
Genu varum is also known as bowed leg is one of the most common deformity to present in Paediatric Orthopaedics clinic.
Physiological varum-When a child is born the legs are bend inward (varum ) till the age of one years, beyond that there is exaggerated valgum till the age of 3-4 years. The legs attains the ‘normal valgus’ by the age of 9-10 years. So, a varum after 3 years of age needs evaluation.
Underlying diseases – rickets ( Vitamin D deficient ), bony dysplasia, growth arrest due to trauma or infection.
Investigations- Always rule out any underlying disease associated with the valgus. A long leg X-ray i.e Hip to toe stitch view is taken in standing position for proper planning and exact localization of the deformity. MRI with cartilage mapping is often required if growth arrest is suspected.
Treatment-
Diagnosis and treatment of the underlying associated disease takes a priority over correction of the deformity. Once the underlying disease is controlled then surgery can be proceeded.
Temporary hemi-ephysiodesis – is the current ‘treatment of choice’ it is a method which works on the principle of utilising the growing potential of a child. A small plate named ‘8’ plate is applied across the physis to temporary stop the growth of one side, on the other-hand the other side of the growth continues and in due course straightens the leg.
Osteotomy– if the growing potential has stopped then correction is done by cutting the bone and straightening the leg.
Role of brace in correction of the deformity– in small child ‘genu-varum’ brace can be applied for small deformities.
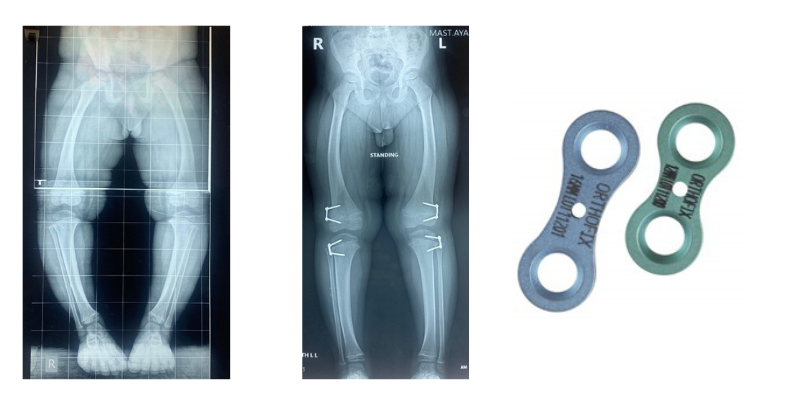
5 year old boy with genu varum corrected by hemi-epiphysiodesis/ growth modulation
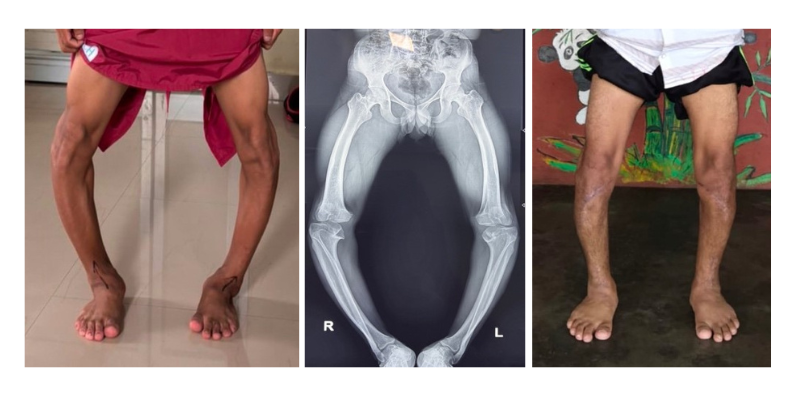
16 year old boy with severe genu varum (spondyloepiphyseal dysplasia) treated with corrective osteotomy